Many people crack their joints on a regular basis, whether out of habit or to relieve stiffness, however, until recently the mechanism that produced this sound has been poorly understood. Historically a number of causes have been proposed including recoil of ligaments or a sudden collapse of gas bubbles within the joint. Most recently a mechanism known as tribonucleation has been proposed which suggests that the rapid formation of gas bubbles within the joint causes the sound. Tribonucleation occurs when two closely opposed surfaces, separated by a thin viscous fluid, are distracted. The tension between the surfaces resist their separation until a critical point where they separate rapidly, creating a cavity (or bubble) within the fluid, much like a solid that has been fractured.
A recent study by Kawchuck et al. (2015) aimed to determine the exact cause of the noise by using real-time MRI on a cracking joint. The Metacarpophalangeal joints (the large joints in your hand at the base of your fingers) were used in the study by inserting the finger into a flexible tube with a length of cable attached that provided traction.
Photo taken from http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0119470
A real-time MRI was then taken as traction was applied to the joint and continued until the cracking event occurred. The results of the study provide evidence that the FORMATION of gas bubbles within the joint causes the sound as opposed to the collapsing of a pre-existing bubble.
But the question still remains, is this cracking bad for your joints? On one hand the energy produced during cracking is enough to cause damage to the joint surfaces, however, research also shows that habitual joint cracking does not appear to show any long term harm. One interesting finding from the study was the presence of a flash of white light on the MRI, just prior to the joint cracking. Kawchuck et al state that further research in this area should help us understand the possible therapeutic benefits, or possible harms, from cracking your joints.
A question I commonly hear in my clinic is “should I change my running style from heel-strike to mid or forefoot-strike?”. My initial recommendation is always do not change your running style just for the sake of it. If you’ve been running for years, and get few injuries you probably have a fairly efficient gait. If you have problems with recurrent injuries look at other factors that may be causing these such as insufficient rehabilitation or training errors (sudden increase in volume, intensity or type of training). Changing your running style is a slow process. When you change a movement pattern in your body it needs to be stored in your muscle memory so you can perform it without thinking, particularly when you are tired. To do this you must repeat the movement many times until it is ingrained in your brain. This takes a long time and in the short term your running economy may reduce as you have to think about how you run.
If you decide that poor running form is a significant causative factor in your injury woes then there are a few points to consider.
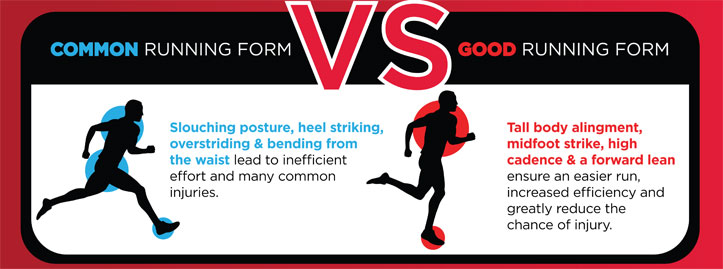
IS FOOT POSITION THE PROBLEM?
There’s more to it than foot position alone. Just because you heelstrike doesn’t mean you have bad form, though runners who heel-strike can often overstride. By moving your footstrike closer to the body a lot of runners will land on their midfoot, however, there are some that will still heelstrike, and that is fine. Likewise there are plenty of mid-foot strikers who overstride. So your focus should be on improving overall running form rather than worrying about your foot position on impact.
HOW DO I IMPROVE MY RUNNING FORM?
Here are 3 simple tips that will help to improve your running efficiency
1. Shorten your stride length
Land with your feet underneath your body rather than out in front. Your knee should be slightly bent. Focus on pushing off rather than pulling forward. You may find that initially you get muscle soreness as your gluts are working much harder than before!
2. Increase your cadence
The optimum steps per minute is 180, however this varies depending on the level of the athlete, and the intensity of your run. First, find your base level by counting the number of steps you take per minute when on an easy run, and then on a tempo run. Add 5% to these totals and these are your initial targets. So if your easy run cadence was 160, aim for 168. If your tempo run was 170 aim for 179. Take care, as upping your cadence too quickly can lead to injury.
3. Keep an upright posture
It is important when incorporating a slight forward lean into your running style that the movement comes from your ankles, and not your back. Don’t consciously try to lean forward, focus on running tall, with a straight posture, and once you shorten your stride a slight forward lean occurs naturally from the ankles.
Photo taken from https://angelajoynutrition.wordpress.com/2015/06/15/improve-running-form/
When looking at the latest research on hamstring injuries I came across an interesting study by Carl Askling and colleagues published in 2013. It compared 2 hamstring rehabilitation programmes, one emphasising strengthening exercises which lengthen the muscle (L-Protocol) and the other using conventional exercises (C-Protocol). The conclusion drawn from the randomised controlled trial was that patients using rehabilitation exercises that concentrated on lengthening the hamstring (eccentric exercises) recovered significantly quicker than those using conventional exercises. Carl Askling also states that of the 190 athletes he has put through his L-protocol rehabilitation programme only 1 has had a recurrence of their injury. This is a pretty incredible recurrence rate of 0.53% compared with normal rates of 12-63% (Brukner et al, 2013).
The L-protocol
The 3 exercises in the programme are commenced 2 days after the onset of injury and performed at specific intervals.
The Extender Performed twice every day for 3 sets of 12 repetitions
The Diver Performed every other day for 3 sets of 6 repetitions
The Glider Performed every third day for 3 sets of 4 repetitions
Once you are fully recovered from your injury it is worth continuing with eccentric exercises as Peterson et al (2011) found a reduced recurrence rate of 85% for patients who continued with a structured programme of Nordic Hamstring Exercises.
A word of warning…the exercises shown on this website shouldn’t be performed before seeing a health professional who can accurately diagnose your injury.
In 1879 a French surgeon first described the existence of a fibrous band on the anterolateral aspect of the knee. Over the years, since then, similar structures have variously been described in the human knee, however, there was no clear anatomical description and its function was unknown. In October 2013 two Belgian knee surgeons published a paper in the Journal of Anatomy describing the structure in detail and have named this ligament the Anterolateral Ligament (ALL).
Dr Claes and Professor Johan Bellemans hypothesis that this new ligament may play an important protective and stabilising role as we twist or change direction. As further research is carried out on the function of this ligament it may help us better understand and treat a very common sports injury – the anterior cruciate ligament (ACL) tear. Despite improvements in surgical techniques around 10-20% of people with repaired ACL tears are unable to recover fully. One of the possible complications after surgery is that the knee will continue to give way as patients twist or turn. Could this be due to the ALL also being ruptured?
At the moment this is all hypothetical and clearly further research is required to elucidate its exact function, but if the ALL is found to have a role in providing rotational stability to the knee, then this may have significant implications for surgery on the knee.
Chronic pain is traditionally one of the most complicated and frustrating disorders to treat, however, recent research and treatment interventions are providing light at the end of the tunnel for many chronic pain sufferers. Research has shown that education about pain is one of the most effective ways of treating it. New treatment protocols which emphasize pain education alongside graded exercise programs are showing excellent results, which can be life changing for the chronic pain sufferer.
So what is pain?
In very simplistic terms pain is a mixture of sensations arriving from nerve endings in the tissues (skin, muscle, tendon, ligament etc) and the interpretation of these sensations by the brain. So for instance, if we touch something hot, nerve endings in the fingers detect the heat and create impulses which travel along a nerve (like an electric current travelling along a wire). These impulses reach the spinal cord and travel up to the brain. The brain then processes these signals and decides what we feel (pain in this instance).
There are 3 different areas in the brain that process pain:
Emotional areas – process how we feel
Cognitive areas – process how we think
Sensory areas – interpret the quality of the sensation (sharp, dull etc)
Recent research has shown that how we think, how we feel, our beliefs, experiences, environment and mood can all influence the severity of pain we feel – the brain can turn pain intensity up. Most people believe pain means damage, however, with chronic pain there is often no underlying injury, yet pain can be felt with everyday activities such as walking or sitting. This is caused by the nervous system becoming sensitised so that the brain perceives a threat to the body with normal activities and initiates a pain response. The brain increases the intensity of this pain so that severe pain can be felt without any underlying damage. A number of factors can play a part in this.
Fear of damage – if you fear that pain is due to permanent damage in your body then you are likely to experience more severe pain.
Fear avoidance – People can become fearful of movement due to pain and concerns about causing damage, so they avoid certain movements and activities. This can lead to muscle weakness and tightness, joint stiffness and increased nerve sensitivity.
Past experience of pain – affects expectation and has a powerful impact on shaping our pain experience.
Hypervigilance – this is a common feature of anxiety and depression which is often associated with chronic pain. People are constantly on the look-out for threats to their body and are constantly aware of any painful symptoms or strange sensations.
Pain focus – constantly focusing attention on your pain is likely to increase pain severity.
Catastrophisation – people who have a negative view of their situation and repeatedly play over their problems in their mind often have poor outcomes. Indeed, Main et al (2010) found that the way someone thinks about pain is a better predictor of pain related disability than the intensity of the pain itself.
Feeling out of control – managing pain isn’t easy and people often feel they have no control over their symptoms. Having pain that you can’t control is worrying and often interpreted by the brain as a greater threat resulting in more severe symptoms.
Stress and low mood – when under stress the body releases an excess of certain hormones which influence how we think and feel. This often results in us experiencing more pain. It is quite common for people’s pain to have a direct link to stress.
Anxiety and depression – Anxiety and depression affect the way we think, feel and behave so that people with mental health conditions often experience more pain. A deterioration in mental health can often coincide with an increase in pain.
Thankfully there are ways in which you can retrain your nervous system to help turn down your pain.
Distraction – our body constantly receives feedback from all over our body, however most of this information is filtered out as it is not deemed useful at that time. For instance, we rarely take notice of how our clothes or shoes feel on our body. Or when we put on a new pair of glasses our body is acutely aware of this new sensation, however after some time we filter this out and forget we are wearing them. Pain can be filtered out in a similar way, especially once we are re-programmed to realize that the pain does not necessarily mean injury!
Pacing – do as much exercise as you can manage without exacerbating your symptoms. For example if you can walk for 5 minutes without any pain, but 6 minutes hurts, then just walk for 5 minutes. This time can slowly be increased as you are able. This puts you back in control of your pain and allows you to stay active so that you no longer associate activity with pain. It also gives you achievable short term goals that you can work towards, such as increasing walking time to 10 minutes. It is important to focus on these short term goals so that you can see progress in your condition
Relaxation – relaxation is an essential element of any pain management programme as it reduces stress, anxiety and catastrophisation. This could be through meditation, progressive muscle relaxation or any formal relaxation technique. Some studies have shown that meditation can reduce chronic pain by up to 50%.
CBT – Cognitive Behavioural Therapy helps people to identify and challenge negative thoughts (eg. pain means damage) and in doing so can improve mood and alter negative behavior (such as fear avoidance).
So there is hope for chronic pain sufferers. With the correct approach that emphasizes education, a graded exercise programme, Physiotherapy and other interventions (CBT, relaxation techniques, meditation) excellent results are now being seen.
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish.AcceptRejectRead More